

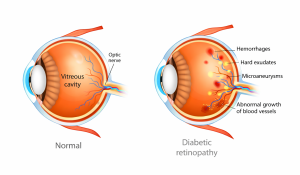
Diabetic retinopathy is a diabetes-related eye condition that affects the retina, the light sensitive layer at the back of the eye, that plays a vital role in vision. It develops when prolonged high blood sugar levels damage the small blood vessels that supply oxygen and nutrients to the retina.
In the early stages, vision may remain unaffected. However, without proper monitoring and management, the condition can worsen over time and lead to vision impairment and in severe cases permanent vision loss.
Diabetic retinopathy develops over time and is classified into two main stages. Each stage reflects the severity of blood vessel damage within the retina.
- Non-Proliferative Diabetic Retinopathy (NPDR)
This is the earlier stage of the condition where small blood vessels in the retina weaken or leak small amounts of fluid, but many patients do not experience noticeable vision changes as symptoms are often absent at this stage. Regular eye examinations play an important role in early detection and allows timely intervention to prevent further progression. - Proliferative Diabetic Retinopathy (PDR)
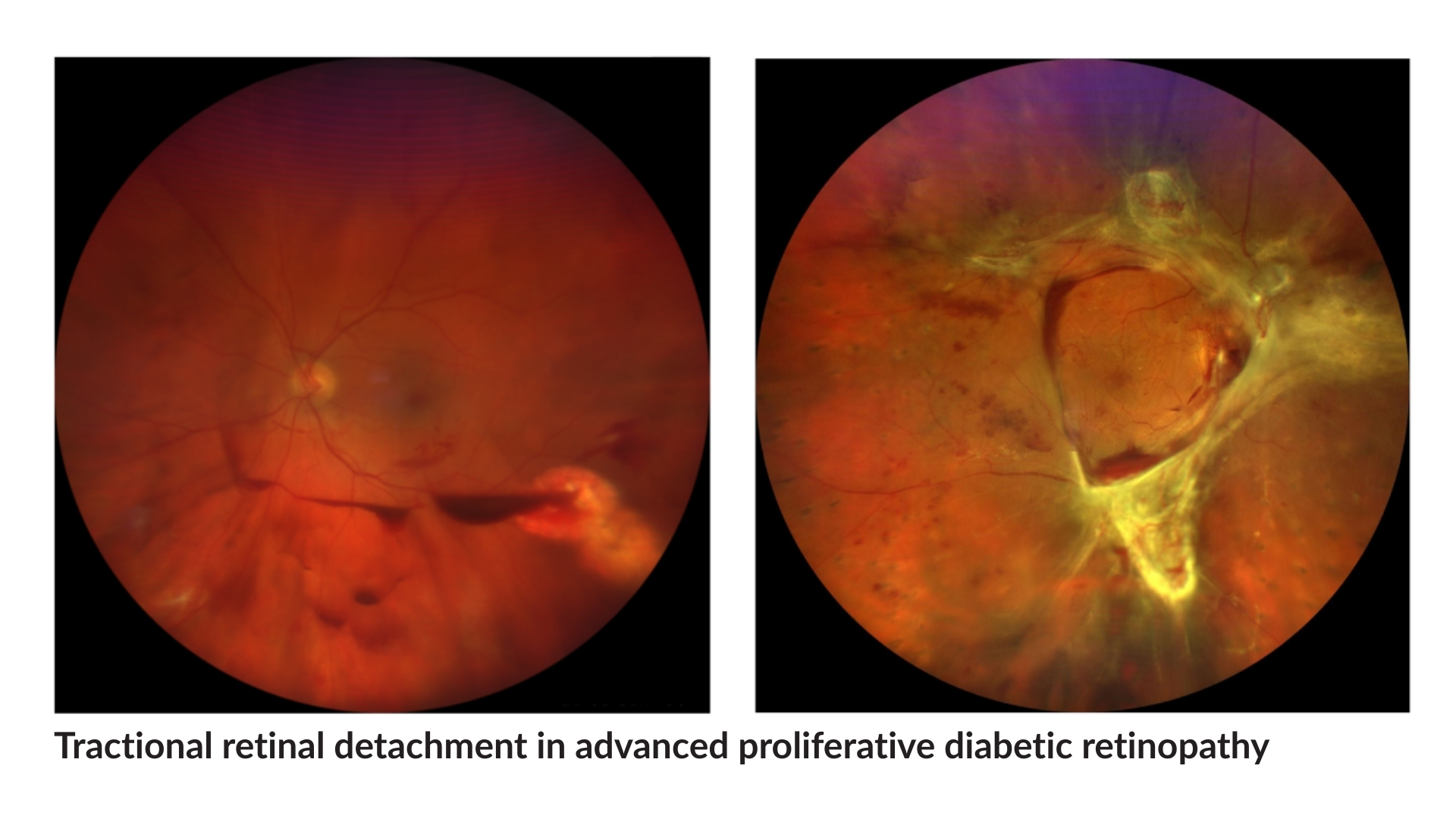
This is a more advanced stage of the disease. When blood supply to the retina is reduced, the eye responds by growing new abnormal blood vessels. These vessels are fragile and bleed more easily, increasing the risk of more severe vision problems such as vitreous haemorrhage, membranes and traction on the retina, retinal detachment, or even high eye pressures.
- Diabetic Macular Oedema (DMO)
When leakage occurs from the retinal blood vessels located in the central part of the retina, i.e. the macula, fluid accumulates amongst the important light-sensing cells responsible for fine and precise vision. This causes vision to become blurry or distorted.



Floaters & Flashes of Light
Sudden appearance of spots, lines, or flashes may indicate changes in the retina and should not be ignored.

Distorted or Wavy Vision
Straight lines appearing bent or distorted can be a sign of macular or retinal conditions affecting central vision.

Blurry Vision
Gradual or sudden blurring of vision may occur when the retina is unable to transmit clear visual signals.
- Ultra Wide-field Fundus Photography
- Spectral Domain OCT
- Fluorescein Angiography
- OCT Angiography

Treatment depends on the severity of the diabetes in the eye, and whether complications of the primary condition have developed. The aim of treatment is to control diabetic retinopathy disease activity, manage and to prevent complications, and to improve and preserve vision.
At Ascend Eye Clinic in Singapore, we offer the following treatment strategies:
- Intravitreal Injections of Anti-VEGF or Sustained-Release Steroid Implants
Medications are delivered through eye injections to reduce retinal swelling and control abnormal blood vessel growth. These treatments are commonly used in moderate to advanced cases.
Several medication options are available, including longer-acting anti-VEGF injections that will allow for fewer treatment visits, and yet still maintain the same level of control of diabetes activity in the eye.
In cases where response to anti-VEGF treatment is limited, steroid implants can be considered as an alternative treatment option, with suitability also depending on the patient’s individual eye condition.
![]()
- Laser Treatment
There are several forms of laser treatment.
Panretinal photocoagulation is used to reduce abnormal blood vessel growth in the entire retina. This approach helps stabilise the condition and lowers the risk of further vision deterioration, and constitutes an important aspect of treatment lending stability to the condition if performed appropriately.
Macular grid and focal laser treatment targets fluid leakage and bleeding at the macula, which is the central part of the retina and responsible for fine and precise vision. The effectiveness can be slightly delayed for a few months, and is a useful adjunct to treatment besides intravitreal therapy.
- Surgical Treatment
In advanced cases, surgery is necessary when bleeding or scar tissue affect the retina or threaten vision. Surgical management of diabetic retinopathy requires careful judgement, precise technique, and experience in handling complex retinal conditions. Advanced cases often involve bleeding, scar tissue, or traction on the retina, which may coexist with other eye problems such as cataract or glaucoma. Management in these situations benefits from a retinal specialist with experience in both medical and surgical treatment planning, so that timing, approach, and follow-up care are appropriately coordinated. - Individualised Long-Term Care
Diabetic retinopathy often requires ongoing follow-up. Treatment plans are regularly reviewed and adjusted to maintain retinal stability and protect vision over time.


