Retinal detachment occurs when the retina, the thin, light-sensing layer at the back of the eye, separates from the eye wall and can no longer function properly. As this separation progresses, vision often becomes blurred, shadowed, or may deteriorate rapidly.
The condition is usually painless, which can delay medical attention , especially if symptoms affect only one eye or the non-dominant eye. Despite the lack of pain, a retinal detachment is considered an eye emergency. Early diagnosis and prompt treatment offer the best chance of preserving vision.
Seek urgent eye care if you notice:
- A sudden increase in floaters (spots, lines, dust, or threads in the vision)
- Flashing lights
- A shadow or curtain in your peripheral vision that spreads toward the centre
- Central vision loss as the central retina becomes involved
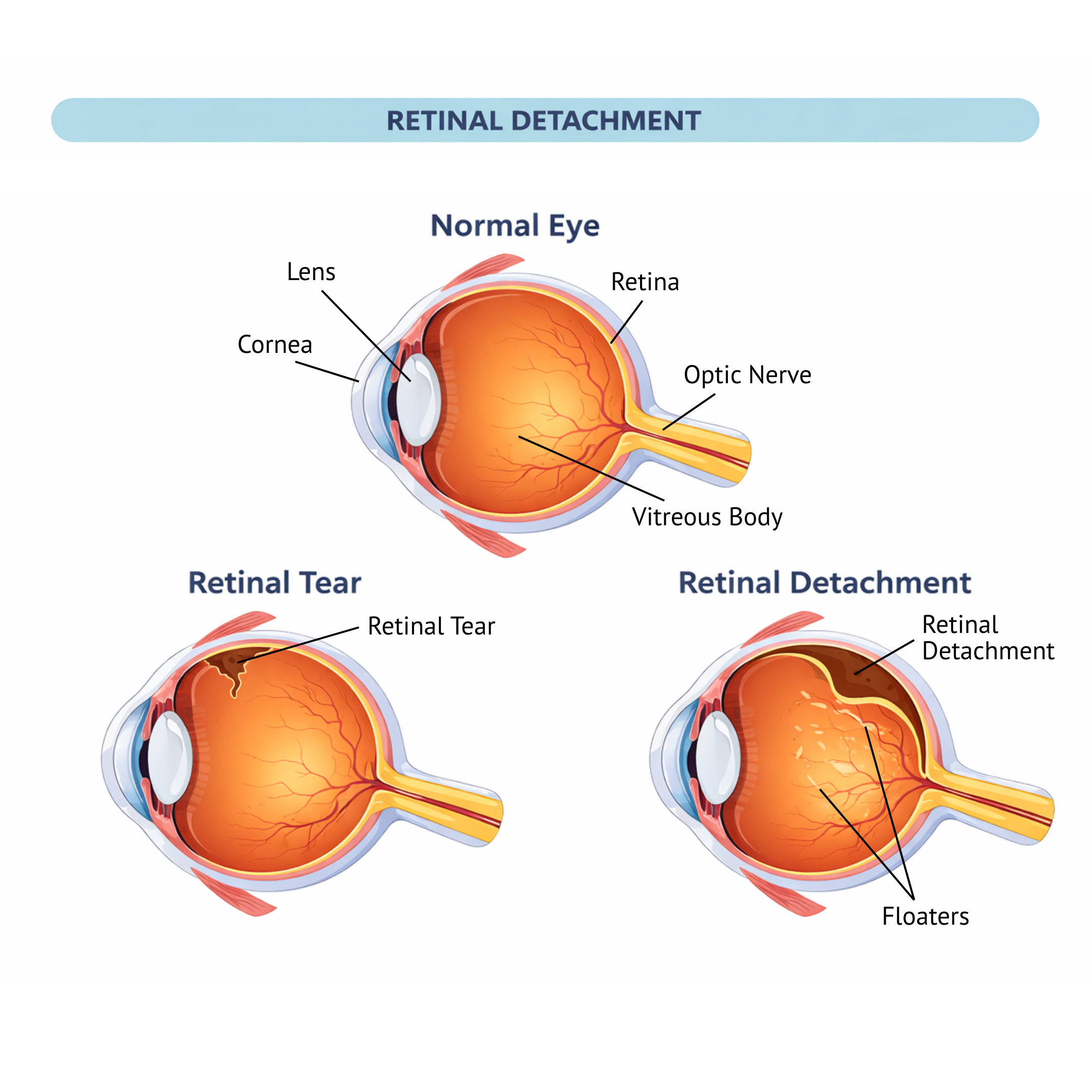


Retinal detachments are grouped into three main types, based on what causes the retina to lift away from the back of the eye.
1. Rhegmatogenous Retinal Detachment
Cause: A tear or hole in the retina, often linked to age-related vitreous changes (posterior vitreous detachment), high myopia (severe short-sightedness), or an eye injury.
What happens: Fluid slips through the retinal tear and collects under the retina, causing it to separate from the eye wall (like wallpaper peeling off the wall). 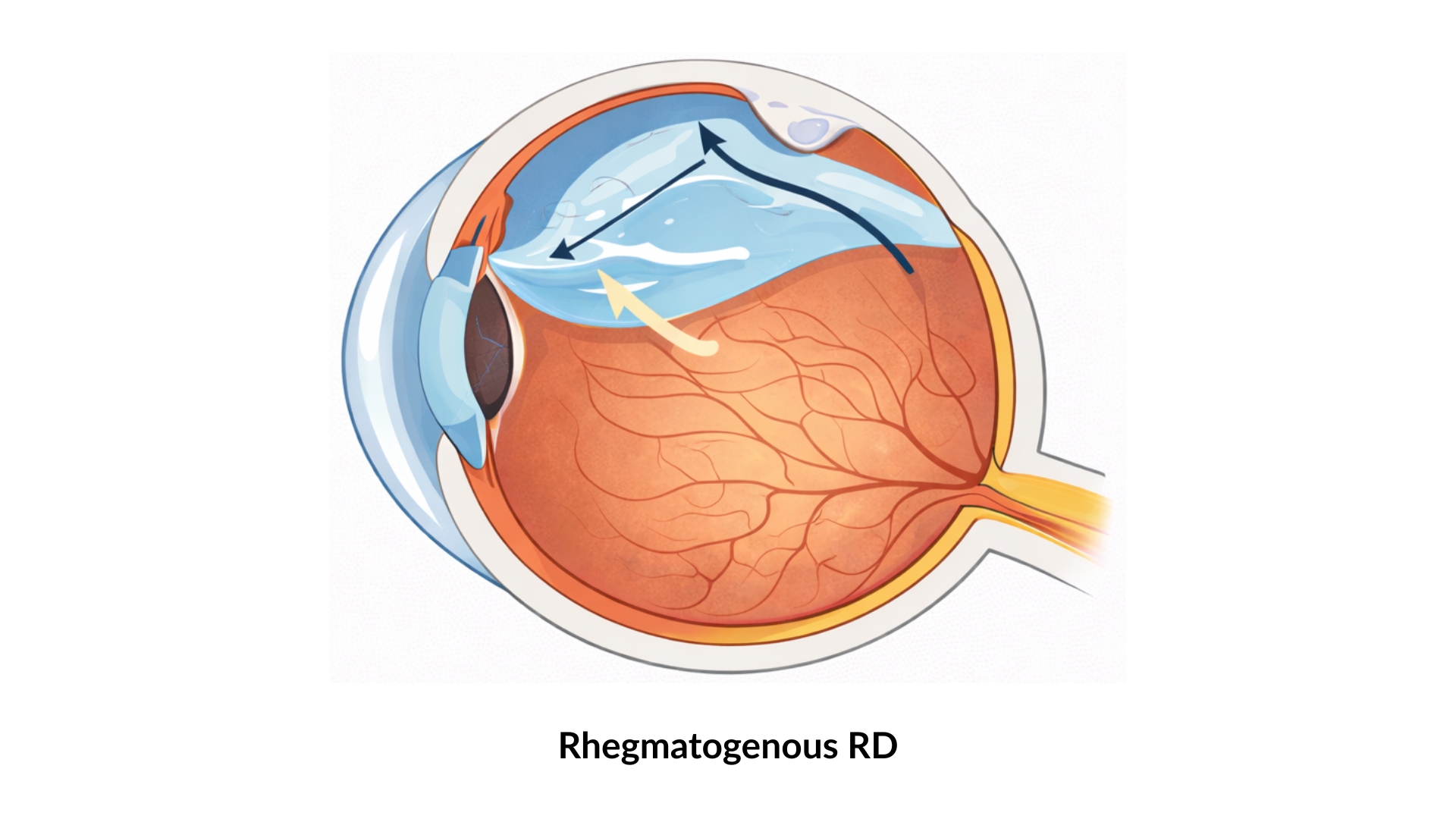
2. Tractional Retinal Detachment
Cause: Scar tissue on the retinal surface, most commonly from advanced diabetic eye disease. The scar tissue tightens and pulls the retina away from the wall of the eye.
What happens: If the pull is sufficiently strong, the retina separates away from its attachment to the wall of the eye, causing a retinal detachment.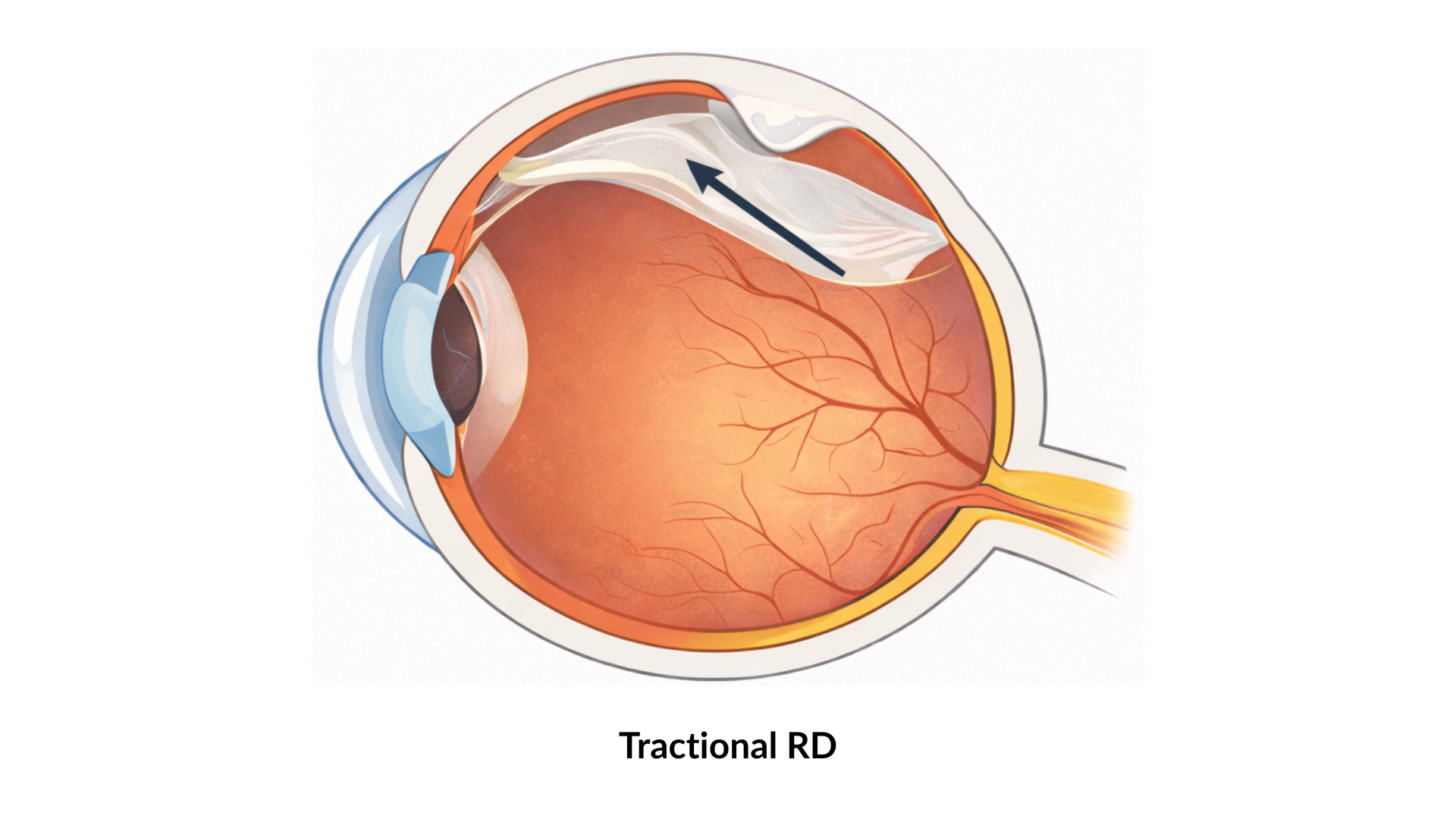
3. Exudative Retinal Detachment
Cause: Fluid leakage beneath the retina due to conditions such as inflammatory eye disease (i.e. uveitis) or leakage from the retinal or choroidal blood vessels.
What happens: Fluid builds up beneath the retina without a retinal hole or tear, causing the retina to separate from the eye wall.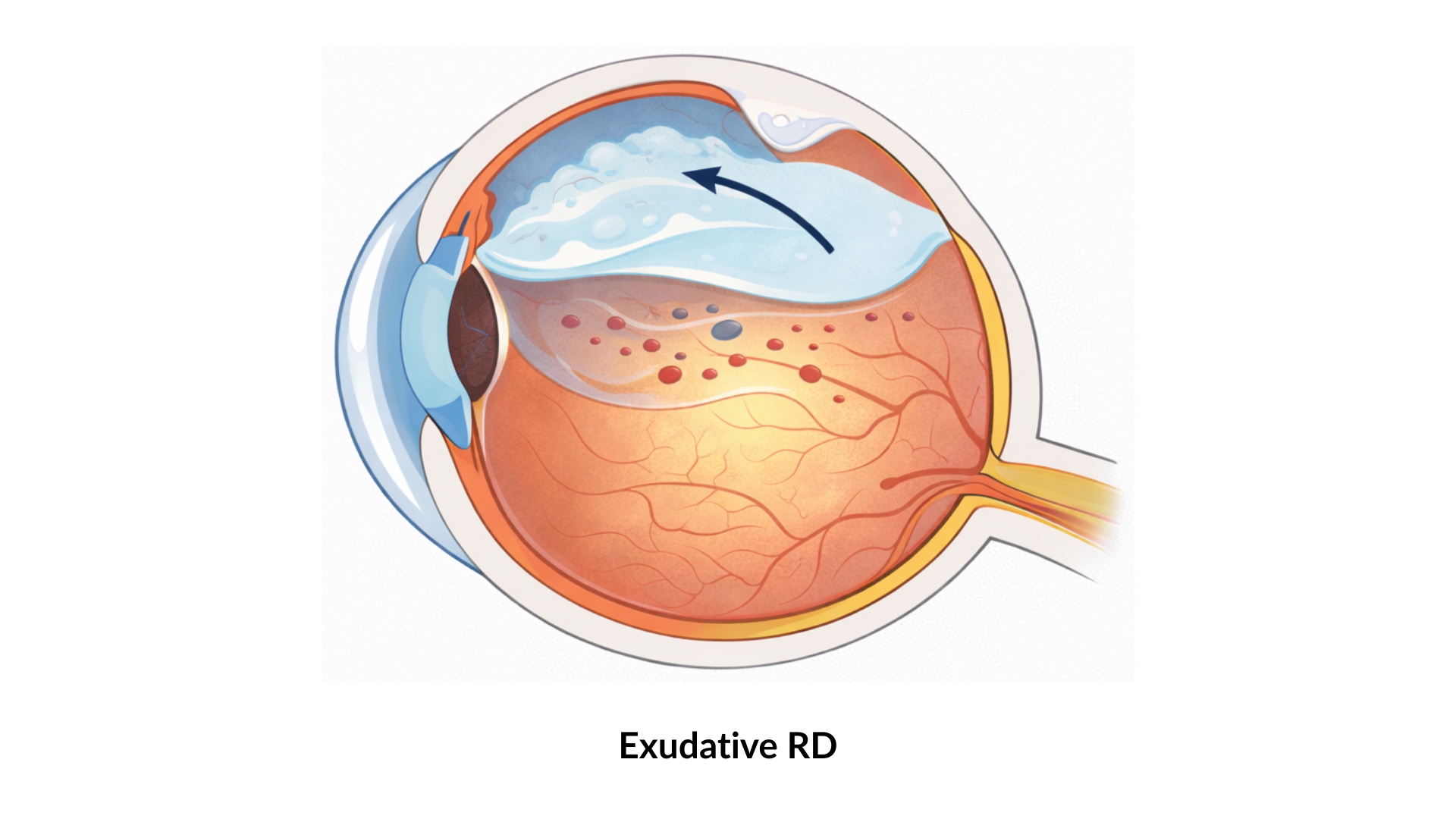
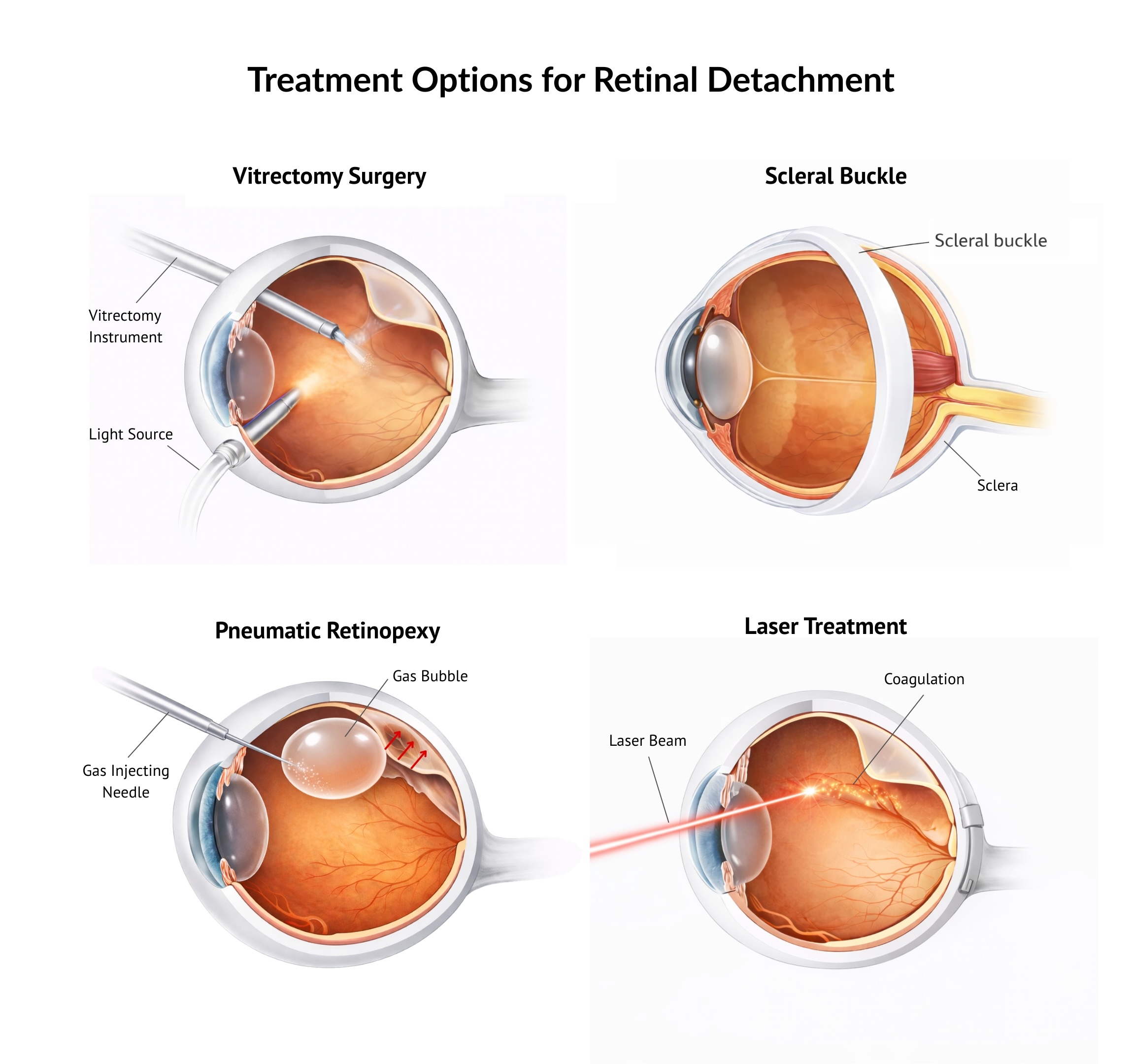
The main goal of retinal detachment treatment is to reattach the retina and seal any tears or holes that have caused it. Several treatment options are available, and the most appropriate approach depends on the type, extent and severity of the detachment, overall prognosis, and individual factors such as age, requirement for air travel, and ability of the patient to adopt specific head positioning postures.
A retina specialist will assess these factors carefully and recommend the treatment that offers the best chance of preserving vision. Modern surgical techniques allow many retinal detachments to be repaired successfully, particularly when treatment is carried out promptly.
- Vitrectomy Surgery
Vitrectomy is a microsurgical procedure where the vitreous gel inside the eye is removed. Fluid trapped beneath the retina is drained, and retinal tears are sealed using laser treatment or freezing therapy (cryotherapy). If there is significant retinal scarring (i.e. proliferative vitreoretinopathy, PVR), then this can be removed. A gas bubble or silicone oil is then placed in the eye to support the retina in position while it heals. - Scleral Buckling Surgery
A soft silicone band is placed around the outside of the eye to gently push the eye wall inward, helping the retina reattach. Retinal tears are sealed with laser or cryotherapy treatment, and in some cases, fluid under the retina is drained. A small gas bubble may also be placed in the eye to provide additional support to the retina for its reattachment. - Pneumatic Retinopexy
A gas bubble is injected into the eye during a clinic-based procedure. The patient maintains a specific head position so the bubble supports the retinal tear. The tear is then sealed with laser or cryotherapy treatment and this allows a permanent seal of the tear. This approach may be suitable for selected cases where the retinal breaks are in the upper parts of the retina, and is therefore considered as an alternative to vitrectomy surgery. - Laser Treatment
Laser therapy is used to create a controlled barricade around the affected area, preventing the retinal detachment from spreading. Laser treatment alone is usually considered for small, peripheral retinal detachments. - Combined Vitrectomy and Scleral Buckling Surgery
In complex retinal detachments or detachments with high-risk features for failure, both procedures may be necessary to enhance the success rates of retinal reattachment surgery.